Ad Disclosure: Some of our MentalHelp.net recommendations, including BetterHelp, are also affiliates, and as such
we may receive compensation from them if you choose to purchase products or services through the links provided
Janet has checked into treatment for the third time. It’s been three weeks, and her detox from alcohol is complete. However, her counselor notices that Janet still appears emotionally flat, seems to be hypervigilant and easily startled, and appears exhausted as a result of vivid dreams that wake her up at night. When she’s startled awake her heart is pounding, and she’s sweating. Janet prefers to spend her free time reading and avoiding the loud teasing and story-telling that the rest of the clients use to bond. If she’s honest, the noise makes her want to bite their heads off, which makes her feel bad about herself. It’s the same reason she avoids her family when she’s home and drinks to “calm down.”
Like many clients in treatment, particularly clients with a multiple relapse history, Janet will continue to struggle with her alcohol use unless the treatment team recognizes that she needs to address the symptoms of Post Traumatic Stress that derail her sobriety.
PTSD and Addiction
Around 50% of individuals seeking substance use treatment also meet criteria for Post-traumatic Stress Disorder (PTSD), and individuals with a co-occurring PTSD/Substance Use Disorder (SUD) tend to have poorer treatment outcomes than those without such comorbidity.1
Evolution and Definition of PTSD
PTSD was initially described as “shell shock” for returning veterans. Our understanding of this painful disorder has evolved in the DSM-5 to identify a broader range of trauma-inducing stressors, including exposure or threat of death, actual or threatened serious injury, or actual or threatened sexual violence. It’s important to identify that the stressor can be experienced directly or by witnessing, indirectly.
DSM-5 Symptoms for PTSD
Symptom patterns are clustered into criterion:2
Criterion A refers to the exposure to actual or threatened death, serious injury, or sexual violence. These can either be directly or indirectly (e.g., learning of a traumatic event of a family member) experienced.
Criterion B includes intrusion symptoms. These may be recurrent or intrusive memories or dreams, and may include flashbacks.
Criterion C includes avoidance symptoms. This is demonstrated by persistent effortful avoidance of distressing trauma-related stimuli after the event (e.g., people, places, conversations, situations) Alcoholism and drug abuse fall into the category of avoidance symptoms, as the individual may use these chemicals to avoid memories or to numb fear.
Criterion D includes negative alterations in cognitions and mood. These changes in mood occur or worsen after the trauma and may include persistent and distorted negative beliefs, self- blame, lack of interest in former interests, feeling separate from others, and feeling emotionally flat.
Criterion E includes alterations in arousal and reactivity that began or worsened after the trauma. These include irritability, recklessness, hypervigilance, exaggerated startle response, poor concentration, and poor sleep.
Criterion F refers to these symptoms lasting more than 1 month.
Criterion G notes that these symptoms must cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Criterion H highlights that these disturbances are not due to the effects of a substance or another medical condition. In other words, the PTSD symptoms arise independently from any physiological effects of using drugs, alcohol, or medication.
Ad
Video: PTSD and Addiction
A great discussion is provided on PTSD and addiction causes, symptoms, and treatments. "Posttraumatic Growth" is discussed, a process whereby those with PTSD experience remarkable growth due to the challenges they have faced.
How Does PTSD Develop?
While research shows that up to 70% of the population has experienced a traumatic event over their lifetime, only about 8% go on to develop PTSD. The key is the perception of helplessness in the face of trauma and prior history of trauma (for example, child abuse). The greater the helplessness, the more likely we are to become trapped in our hyper-arousal cycle and later develop posttraumatic symptoms.3
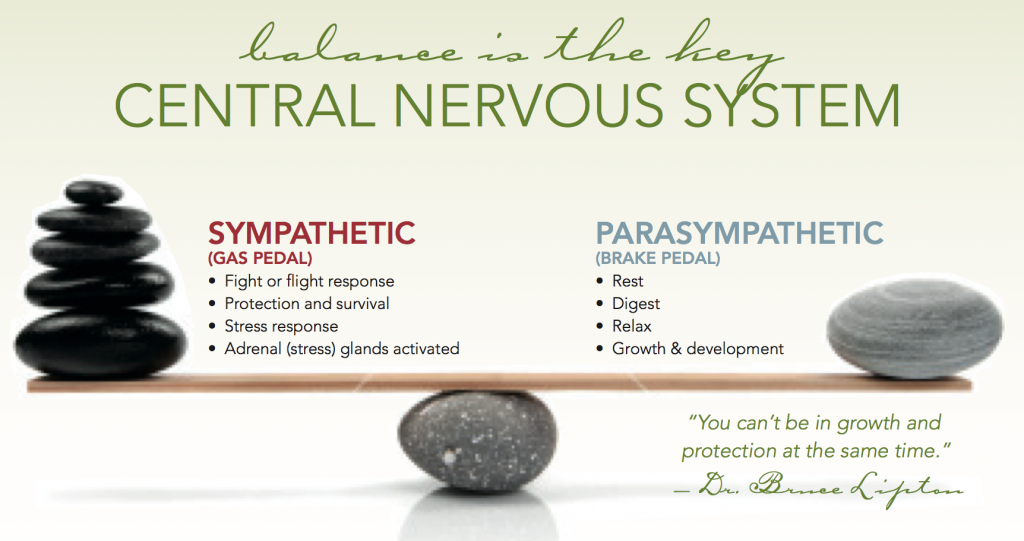
When we encounter stress, our sympathetic(“fight, flight, or freeze”) system responds, our adrenal system is triggered, cortisol is released, and our body becomes
prepared to move toward the threat (fight), move away from the threat (flight), or we may even dissociate(freeze). Afterward, our parasympathetic (“rest, digest, and heal”) system takes over, and our bodies are restored to “normal” functioning.
In PTSD, we do not fully return to the parasympathetic system and are therefore always primed for a fight-flight-freeze reaction. We are never fully at rest, always vigilant and may have distorted perceptions of threat. An analogy might be to keep your foot on the gas pedal without letting up. Sooner or later the engine will begin to burn out. It is not uncommon for PTSD suffers to develop accompanying stress-based disorders such as fibromyalgia, chronic fatigue, clinical depression, or colitis. A sizeable portion also go on to develop an addiction.
The Role of Addiction in PTSD
Chemical dependency is often described as an attempt at self-regulation, not so terribly different from self-injury other types of trauma-related impulsive behavior. From this perspective, we come to see that addiction is a result of an attempt to ward off the intrusive memories, smooth out hypervigilance, and disconnect from anxiety.
When alcohol or drugs are used to manage PTSD symptoms, the symptoms of the disorder only become more severe. As a central nervous system depressant, alcohol and opiates can worsen depression and anxiety and interfere with normal sleep patterns.
We might mistakenly believe that treating the trauma will stop the alcohol and drug abuse. However, addiction may continue to persist given that the substance has hijacked our reward system, causing us to develop enduring tolerance (need more of the substance to get the same effect) and withdrawal (physical consequences and discomfort when substance use stops) symptoms.
For these reasons, addiction issues must always be addressed concurrently in trauma recovery, because the substance abuse will consistently undermine all other treatments by impairing our memory, perception, and judgment.
Similarly, trauma issues should always be addressed concurrently in addiction recovery, given that the presence of trauma symptoms makes substance abuse much more likely.
Successful recovery requires clients to understand how the addictive substances have helped them survive: that is, which trauma symptoms have they been attempting to treat through drinking and drugging? We need to know this because the trauma symptoms will increase when we enter sobriety, and we will need coping strategies to manage the triggers of PTSD when they appear. Relapse prevention plans must create strategies to manage both addiction and PTSD symptoms and triggers.
Trauma-Informed Treatment
Successful trauma-informed treatment might include combinations of:
Psychoactive medication, if necessary, to address hyperarousal.
Mindfulness and distress tolerance skills to address arousal and disconnection from the self.
Cognitive Behavioral Therapies to address the distortions in thinking that occur as a symptom of both addiction and PTSD.
Both inpatient and outpatient treatment centers may offer these options. Be sure to ask the treatment provider if they treat co-occurring trauma and addiction.
Janet’s counselor had recently completed a co-occurring disorder course and recognized the significance of Janet’s history of domestic violence leading to her husband's 5-year prison term. Janet had not considered the impact of the violence on her use of alcohol because he’s incarcerated. However, her symptoms continued to persist and were influencing her drinking habits.
It was not in the scope of practice for Janet's CADC counselor to treat her PTSD, but she asked Janet about her symptoms and was able to make a referral to a local mental health counselor and psychiatrist who often treat substance abusers with mental health issues. Also, her counselor placed Janet in the program's “Seeking Safety” group, gave her an information sheet about PTSD so that Janet could see that she wasn’t just “crazy,” and encouraged Janet to keep a journal of her PTSD symptoms triggers along with her alcohol triggers. When it comes time to write Janet's relapse prevention plan she will write the plan for both PTSD and addiction management. Addressing both of these disorders together will increase Janet’s likelihood of finding sobriety and greater health.
Resources
Brady, K. T., Back, S. E., & Coffey, S. F. (2004). Substance abuse and posttraumatic stress disorder. Current Directions in Psychological Science,13(5), 206-209.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edition: DSM-5 5th Edition (DSM-5). Arlington, VA: American Psychiatric Association.
Joseph Volpicelli, M.D., Ph.D.; Geetha Balaraman; Julie Hahn; Heather Wallace, M.A.; and Donald Bux, Ph.D. The Role of Uncontrollable Trauma in the Development of PTSD and Alcohol Addiction. (1999). Alcohol Research & Health, Vol. 23, No. 4, pgs 256-262.
Substance Abuse and Mental Health Services Administration (SAMHSA). Trauma-Informed Approach and Trauma-Specific Interventions. Retrieved at http://www.samhsa.gov/nctic/trauma-interventions
Additional Resources
As advocates of mental health and wellness, we take great pride in educating our readers on the various online therapy providers available. MentalHelp has partnered with several thought leaders in the mental health and wellness space, so we can help you make informed decisions on your wellness journey. MentalHelp may receive marketing compensation from these companies should you choose to use their services.
Talkspace Online Therapy & Psychiatry - Licensed therapists and psychiatrists are available for virtual sessions via Talkspace. From virtual counseling to medication management services, Talkspace online therapy may be covered by your insurance provider. Simply fill out a brief assessment online to save $100 and match with a licensed therapist today.
MentalHelp may receive marketing compensation from the above-listed companies should you choose to use their services.